





 69 / 224
69 / 224

783
(though this was not statistically significant in this series).
Lenarz et al. (16) also provided data for listening in noise
performance in a smaller subset of subjects, which showed
very similar patterns to those demonstrated for monosylla-
bles in quiet.
Skarzynski and colleagues have reported extensively on
outcomes from implantation of subjects with a range of
different levels of low frequency hearing (19,26). They
classified potential CI recipients according to the level of
preoperative low frequency thresholds. Thus, “electric
complement” subjects (Group A) had 500 Hz thresholds
better than 50dB HL and did not always require any acoustic
amplification. “EAS” subjects (Group B) had 500 Hz thresh-
olds of 50–80dB HL and would be anticipated to utilize
acoustic amplification and electrical stimulation in the
implanted ear, and “electrical stimulation” subjects (Group C)
had 500Hz thresholds outside the range that might benefit
from amplification (
>
80dBHL), i.e. conventional CI candi-
dates.
In a series of 35 subjects implanted with the Cochlear
CI422 (with Slim Straight electrode array), this centre used
a partial insertion (20–23mm) for Group A and B subjects
and a full 25mm insertion for Group C subjects (26).
Outcomes for the Group C subjects (n=11) were comparable
to those obtained in conventional CI candidates with other
full length electrode arrays. Of the two groups of potential
electro-acoustic stimulation users, there were 11 and 13
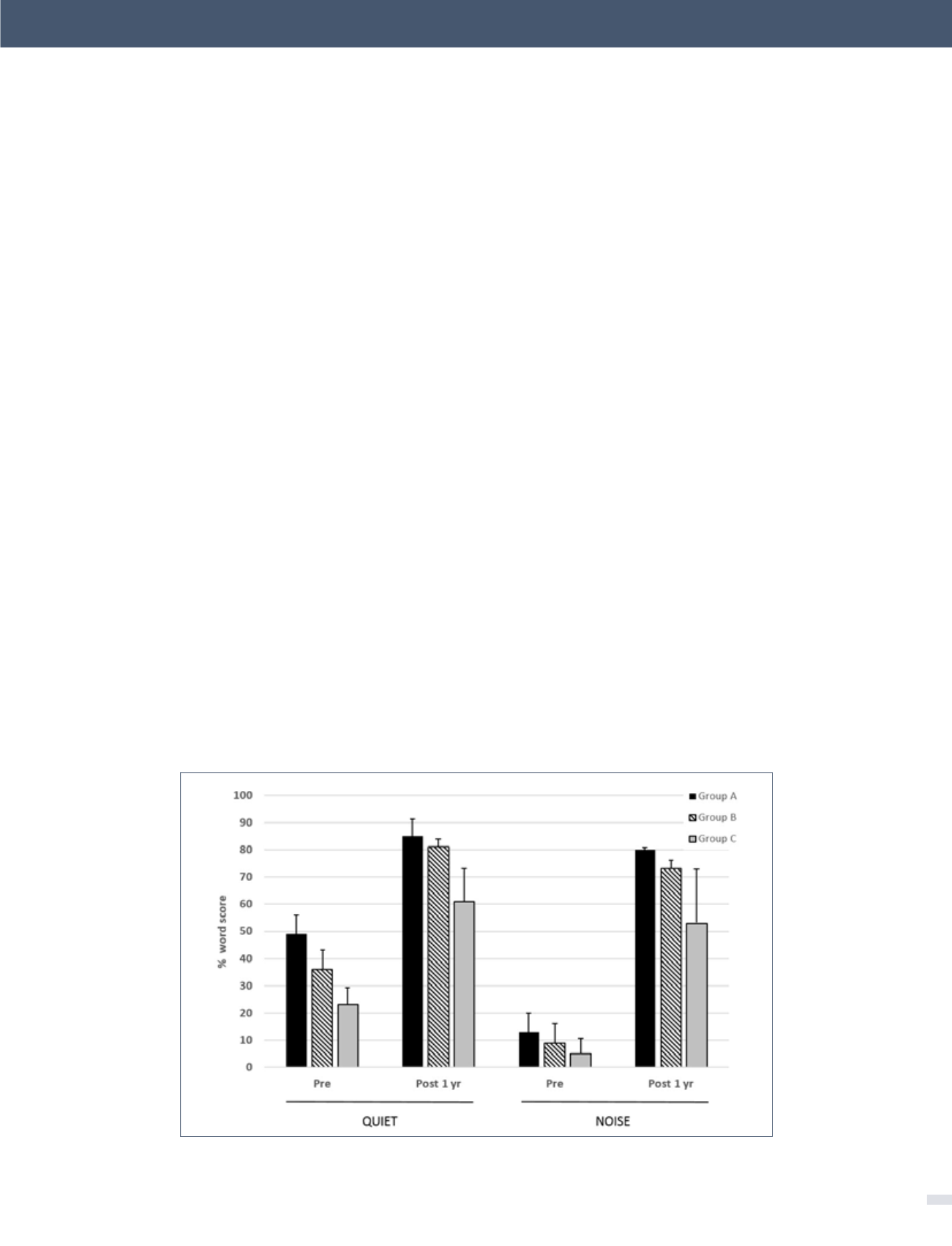
subjects in Groups A and B respectively. Figure 6 shows the
1 year scores for the three groups tested on monosyllabic
words in quiet and in speech-shaped noise (10dB signal-
noise ratio). The added benefit of acoustic input is evident
from the significantly higher scores in Groups A and B rela-
tive to those of the Group C subjects. Greater post-implant
improvement is evident in noise as compared with in quiet
for all three groups.
Functional consequences of loss of residual hearing
As outlined in the previous section, there is evidence of
an increased risk of a major loss of residual hearing with
longer electrode arrays, either at the time of surgery or over
the subsequent months or years. The use of short arrays
tends to result in slightly better hearing preservation, but
a very short electrode may not provide equivalent CI-alone
performance to longer arrays. When loss of functional
hearing occurs, the CI user only has access to information
delivered electrically to the implanted ear. There are reports
of small numbers of recipients of the 10mm Cochlear Hybrid
S device who lost residual hearing and received limited
benefit in the CI-alone condition. Some of these subjects
were subsequently re-implanted with standard Contour
arrays, with improved outcomes in both the CI-alone and
“best aided” conditions (14,42).
Friedmann et al. (21) assessed the functional effects of loss of
residual hearing in a cohort of Cochlear CI422 and Hybrid L
recipients. Median low frequency threshold loss after
figure 6. Mean 1 year post-implantation monosyllable scores in quiet and 10
dB SNR noise for three groups of subjects implanted with the Cochlear CI422
Error bars show standard deviations. See text for further details. (from Skarzynski et al. (26) with permission).
[Electro-Acoustic Stimulation - an option when hearing aids are not enough - Herbert Mauch Biomed Eng. et al.]