














 58 / 176
58 / 176

702
Short-term central venous access
There is a wide choice of devices typically inserted via
guidewire techniques. Commoner devices include; standard
multilumen central venous catheters (CVC), a ‘long line’ or
peripherally inserted central catheter (PICC), valved intro-
ducer sheaths, and dialysis-type catheters.
A range of fixed lengths is needed to suit each insertion
site. For adults, use 15cm for the right internal jugular vein
(IJV), 20cm for the left IJV and right axillary/subclavian
vein, and 24cm for left axillary/subclavian and femoral
veins. Use the narrowest gauge suitable to reduce inser-
tion trauma. Large-bore catheters and dilators devices do
not traverse corners easily, so use right IJV or femoral veins
if possible. Compare the size of a vein on ultrasound with
the catheter diameter. A catheter occupying more than
1/3
rd
of the diameter is associated with increased risk of
thrombosis
ROUTES OF ACCESS
Internal jugular vein
Right side access is linked to lower insertion complications
and tip malposition. There is variation in carotid artery and
IJV relation, and a dominant vein on one side. In sicker
patients there is increased risk of infection due to prox-
imity of oral secretions. Carotid puncture or catheterisation
should be avoidable with ultrasound. Arteries like the thyro-
cervical trunk and branches, vertebral, and subclavian lie
behind the vein (Figure1) and can be hit on vein transfixion.
•
Local or systemic infection
•
Thrombosed, painful veins
•
Leakage of fluids into tissue leading to:
-Ineffective drug administration,
-Drug extravasation with skin/tissue loss
•
Compartment syndrome from pressurized infusions
•
Inadvertent arterial cannulation
•
Catheter fracture or damage.
TABLE 1. COMMON COMPLICATIONS OF PERIPHERAL
CANNULATION
•
Monitoring of central venous pressure
•
Large-volume fluid resuscitation
•
Parenteral nutrition.
•
Drug administration
•
Pacing wires
•
Insertion of pulmonary artery catheters
•
Dialysis/haemofiltration
•
Lack of peripheral access
•
Cardiopulmonary bypass
•
Drug administration
TABLE 2. INDICATIONS FOR CENTRAL VENOUS ACCESS
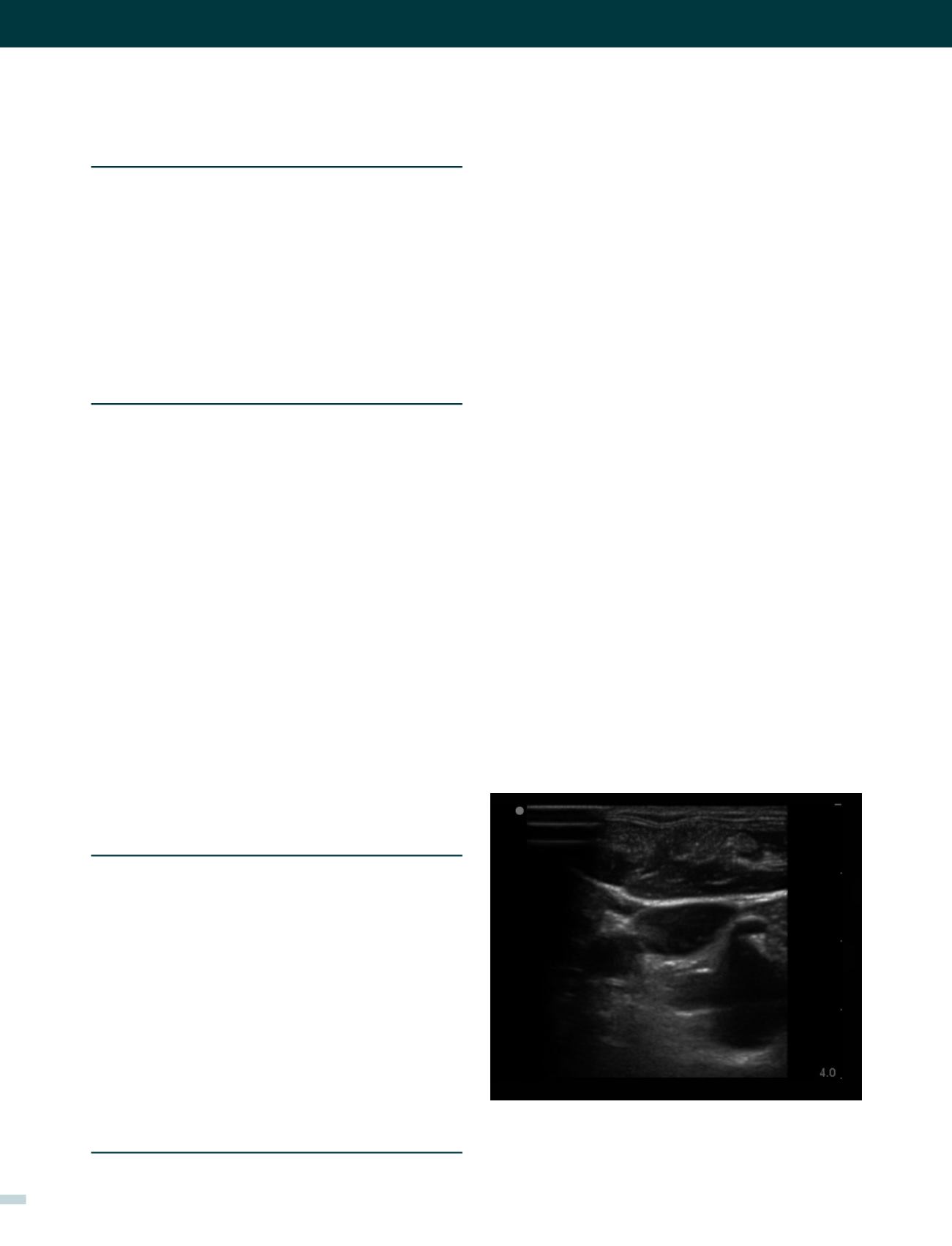
FIGURE 1. AN ULTRASOUND IMAGE OF RIGHT IJV LOW
IN THE NECK
Intraosseous injection
This route of access is widely used in adult and paediatric
resuscitation. A needle with a trocar is inserted into the upper
tibia to access venous sinuses. There are purpose-designed
needles and powered drills available. Care must be taken to
avoid extravasation, bony injury, and infection, and standard
venous access should be sought soon after (8).
Central venous catheters
Many patients will require central venous catheterization
in short or longer term (Table 2). More than an estimated
250000 are inserted annually in UK. Contraindications
are relative including; limited sites for access, anatomical
variants, venous stenosis, previous difficulties/complica-
tions, severe coagulopathy, and local sepsis at the inser-
tion site.
Note the close proximity of the subclavian artery (and its branch the
thyrocervical trunk) which is close behind and vulnerable to damage from
needle transfixion of the vein.
[REV. MED. CLIN. CONDES - 2017; 28(5) 701-712]